

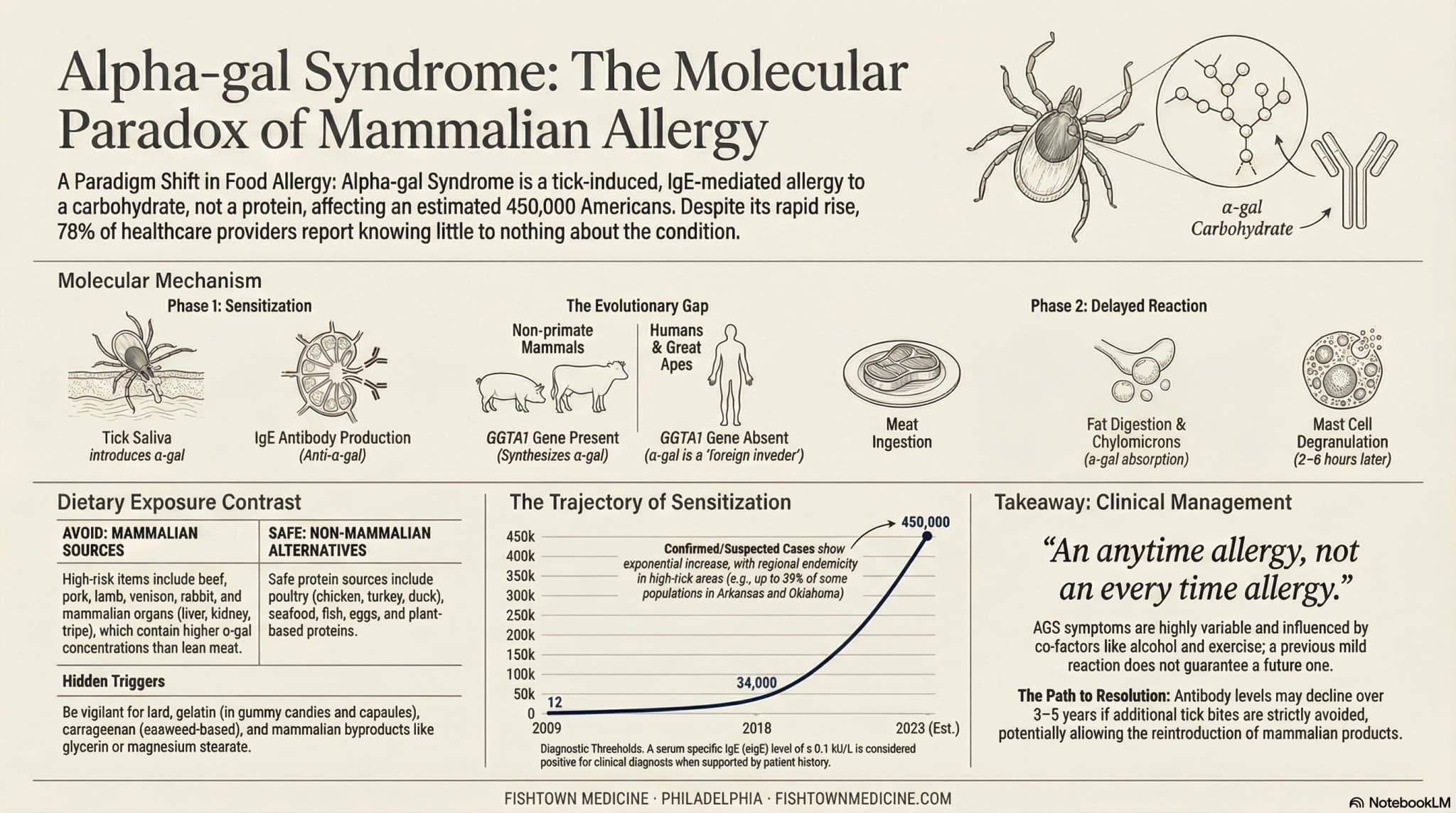
Alpha-gal syndrome is a tick-triggered allergy to mammalian meat caused by a sugar molecule called galactose-alpha-1,3-galactose. The classic pattern is delayed reactions (3 to 6 hours after eating beef, pork, or lamb), often waking patients at 3 AM with cramping, hives, or anaphylaxis. The serum alpha-gal IgE blood test diagnoses it, and the lone star tick that causes it is now established across the Delaware Valley.
Why is alpha-gal syndrome now a Delaware Valley problem?
Alpha-gal syndrome is now a Delaware Valley problem because the lone star tick has expanded its range. It used to be a Southern story, and it is not one anymore. Most of Pennsylvania is in the active range now, along with all of South Jersey and Delaware. The tick rides an expanding white-tailed deer population and warmer winters into the places our patients spend their time: the Wissahickon, Pine Barrens sand roads, Bayshore marshes, and the beach grass down the shore.
If you are someone who runs, hikes, gardens, hunts, or walks a dog off-leash anywhere green in this region, then yes, you are in the exposure zone. The tick does not care that Philadelphia has been a Lyme city for 30 years.

A lot of local rheumatology and GI practices are still working off a mental map from 10 years ago, and we do not blame them for it. When you are seeing a patient every 7 minutes and the insurance is deciding what you can order, a newly migrating tick borne allergy is not going to make the top of your differential. But the map is wrong now. Alpha-gal is not a Carolina problem anymore.
What is the alpha-gal syndrome pattern that keeps getting missed?
Here is the tell. Somebody who has been eating burgers their whole life has a steak dinner, sleeps fine for a while, then sits up in bed around 3 AM with cramping or nausea or whole body itching. Sometimes hives. A lot of the time, no hives at all. The delay is the strange part, and it comes down to how the allergen travels. Alpha-gal rides on fat, and fat takes a few hours to clear digestion and get into the bloodstream. That is the 3 to 6 hour window everybody talks about.
About 1 in 5 of these patients never get hives. They just get the gut version, which is why so many of them end up parked in a gastro office being told they have IBS. Scopes, CT scans, low-FODMAP, the whole tour. The national average to a correct diagnosis runs about 7 years, which is almost all of elementary school spent reacting to dinner.
Here is the order entry trap, and we have watched smart docs trip on it. Alpha-gal IgE gets confused with alpha-galactosidase, a separate test for Fabry disease. It is a different test for a different disease, so spell it out when you order.
The blood test by itself is not the diagnosis. You need the test and a story that fits. Skin prick testing with commercial meat extracts misses alpha-gal a lot, so do not use it to rule this out.
Why is "avoid red meat" wrong advice for alpha-gal syndrome?
Most patient handouts stop at beef, pork, and lamb. We get it, the doctor writing that handout had 7 minutes with the patient and an inbox full of prior authorizations. But incomplete advice is why so many alpha-gal patients keep reacting after they think they have already fixed their diet.
First thing they miss: fat and organs. Alpha-gal lives in fatty tissue, so a lean cut of beef and a bowl of refried beans cooked in lard are not in the same risk category. Organ meats are the worst on this front. Liver, kidney, tripe, sweetbreads, all of them. The sneaky exposures, the ones that get people who already think they are being careful, are tallow in restaurant fry oil, gelatin in gummy vitamins and marshmallows, carrageenan in almond milk and packaged lunch meat. None of those say "red meat" on a label.
Then there is the co-factor problem, which may be the most underappreciated part of this disease. Somebody who handles a small burger on a Tuesday and feels fine can have a much worse time with the same burger if they:
- had a couple drinks with dinner
- took ibuprofen earlier in the day (or any other NSAID)
- did a hard workout that afternoon
- slept badly the night before
- are coming down with something
These co-factors pull a lot of weight. They can turn a subthreshold exposure into an ER visit. Anybody with a positive alpha-gal IgE should be taught the co-factor list as much as the food avoidance sheet before they are sent home.
The exposure we lose the most sleep over is the medicine cabinet.
Over 60% of the drugs in the FDA DailyMed database contain at least one potentially mammal derived ingredient once you count the inactive excipients (gelatin, magnesium stearate, lactose, glycerin). Most alpha-gal patients will not react to trace amounts. A small subset of highly sensitive patients reacts even to those. If somebody with a clear diagnosis keeps reacting to things they "shouldn't," walk the medication list through with a pharmacist before you conclude the diagnosis is wrong.
Who should not get tested for alpha-gal syndrome?
Fishtown Medicine
A 90-minute conversation with Dr. Ash. A written plan you can actually follow.
The test is cheap. The diagnosis is the hard part, because it is clinical. A positive lab without a history that fits is only a data point until the story lines up behind it. So we are not chasing alpha-gal IgE on every belly ache.
Skip the test if there is no tick exposure history, no delayed reactions, and nothing gut related tied to meat specifically. A positive in that setup is almost always asymptomatic sensitization, which lots of people carry and never notice.
Skip it if reactions kick in within 30 minutes of eating. That points to a classic protein allergy, a different mechanism with a different workup.
Skip it, too, if the reactions track with specific preparations (a marinade, a rub, grill smoke) rather than the meat itself. That one needs its own investigation.
Here is one more uncomfortable number. In lone star tick country, something like 15 to 20% of adults already carry detectable alpha-gal IgE and have no clinical allergy. A 2026 blood donor screen by Dr. Scott Commins's group at UNC found that in Arkansas, Kentucky, and Missouri, nearly 30% of random donor samples were antibody positive. Most of those people will never react to a burger, so the test only means something when you already have a story pointing at it.
What should I ask my doctor about alpha-gal syndrome?
If the pattern we have been describing sounds familiar, do not try to memorize a script. You only need to get a couple of points across to whoever you are talking to. Pick whatever fits.
The first one is the test name itself, which is the part that gets fumbled most. Ask for a serum alpha-gal IgE, by name, and tell them it is not the alpha-galactosidase enzyme assay (that is Fabry disease). They are two different tests, one letter apart in the order menu, and people mix them up.
The second is about safety while you are figuring this out. If you have already had a hard reaction, that conversation should include whether you go home with an epinephrine auto-injector tonight or wait. We usually say yes if there has been any systemic component.
The third is documentation, and people skip it. Get alpha-gal logged on your chart allergy list, the same place a penicillin allergy would live. That is what flashes red in front of an anesthesiologist or an ER doc before anyone hands you a vaccine or rolls you back for a procedure.
Fourth, and this is the boring one that saves people a lot of grief: ask a pharmacist to walk through your current med list and check the inactive ingredients, which are the ones people forget. You want eyes on gelatin, magnesium stearate, glycerin, the works.
Last, ask about retesting in a year if you stay tick free. Most people do not realize this, and it is the hopeful part of the whole story. Alpha-gal IgE drops over time in people who stop getting bitten, and a fair share of patients get back to tolerating meat after 1 to 5 years of strict tick avoidance. So prevention does more than keep you from feeling sick tonight. It is the road back to a steak in 2030.
Actionable Steps for Patients Who Suspect Alpha-Gal
- Order the right test by name. Serum alpha-gal IgE. Not alpha-galactosidase. LabCorp or Quest. Cost is typically under $50.
- Start a reaction journal. Three columns: what you ate, when you ate it, and what else was going on (alcohol, NSAIDs, exercise, illness, sleep).
- Get an EpiPen prescription if you have had any systemic reaction (whole body itching, throat tightness, vomiting plus rash, or fainting).
- Get alpha-gal added to your chart allergy list if positive.
- Walk your med list through with a pharmacist to identify gelatin and other mammal derived ingredients.
- Buy permethrin and treat your outdoor clothing before the next hike.
One last thing from clinic. The alpha-gal patients who claw their way back to normal are the ones who stop getting bitten, more than the ones who perfect their diet. Diet controls the reaction you have tonight. Tick avoidance decides whether you still have this thing in 2031. The two do different jobs, and both matter.
So if you live somewhere between the Schuylkill and the Atlantic, spend much time outside, and you have had one strange midnight reaction to a meal you have eaten a thousand times, the alpha-gal IgE is worth running. If you have been carrying an IBS label that never quite added up, same answer. The cost of being wrong is a normal lab. The cost of being right is the rest of a decade of unexplained symptoms making sense at last.
Scientific References
- Commins, S. P., et al. (2009). Delayed anaphylaxis, angioedema, or urticaria after consumption of red meat in patients with IgE antibodies specific for galactose-alpha-1,3-galactose. Journal of Allergy and Clinical Immunology, 123(2), 426-433.
- Carson, A. S., et al. (2023). Tick-Associated Mammalian Meat Allergy: Current Understanding and Diagnostic Approach. Mayo Clinic Proceedings, 98(4), 568-580.
- Steinke, J. W., Platts-Mills, T. A., & Commins, S. P. (2015). The alpha-gal story: lessons learned from connecting the dots. Journal of Allergy and Clinical Immunology, 135(3), 589-596.
- Centers for Disease Control and Prevention. (2023). Alpha-gal Syndrome Subcommittee Report to the Tick-Borne Disease Working Group.
- Wilson, J. M., et al. (2019). Investigation into the alpha-gal syndrome: characteristics of 261 children and adults reporting red meat allergy. Journal of Allergy and Clinical Immunology: In Practice, 7(7), 2348-2358.
- Wilson, J. M., Nguyen, A. T., Schuyler, A. J., et al. (2018). IgE to the mammalian oligosaccharide galactose-alpha-1,3-galactose is associated with increased atheroma volume and plaques with unstable characteristics. Arteriosclerosis, Thrombosis, and Vascular Biology, 38(7), 1665-1669.
- Binder, A. M., Commins, S. P., Altrich, M. L., et al. (2023). Diagnostic testing for galactose-alpha-1,3-galactose, United States, 2010-2018. Annals of Allergy, Asthma & Immunology, 130(4), 411-417.

Frequently Asked Questions
Common Questions
Deep-Dive Questions
Ready when you are
The chat is our AI assistant, answering from our published guides. To talk it through with Dr. Ash himself, schedule the free 20-minute call.


